
About IHF
The Bricklayers and Allied Craftworkers International Health Fund was established in 1988 by the International Union of Bricklayers and Allied Craftworkers and various Contractor Associations. It is financed by employer contributions established in collective bargaining agreements between the Union and employers participating in the International Health Fund (IHF).
The Trust Fund is separate from, and not a part of, the International Union or any employers' association. The U.S. Treasury has advised that the Fund is exempt from Federal income taxes under provisions of Section 501(c)(9). Members are covered by the Health Plan if they are an employee working under a collective bargaining agreement between an employer and the Union providing for contributions to this Fund.
International Plan
We are an International Plan covering members in 41 states 4 Canadian Provinces.

IHF Private Exchange
The International Health Fund (IHF) offers participating Locals access to quality medical, hospital and other health benefits for their members at competitive rates through the IHF Private Exchange.
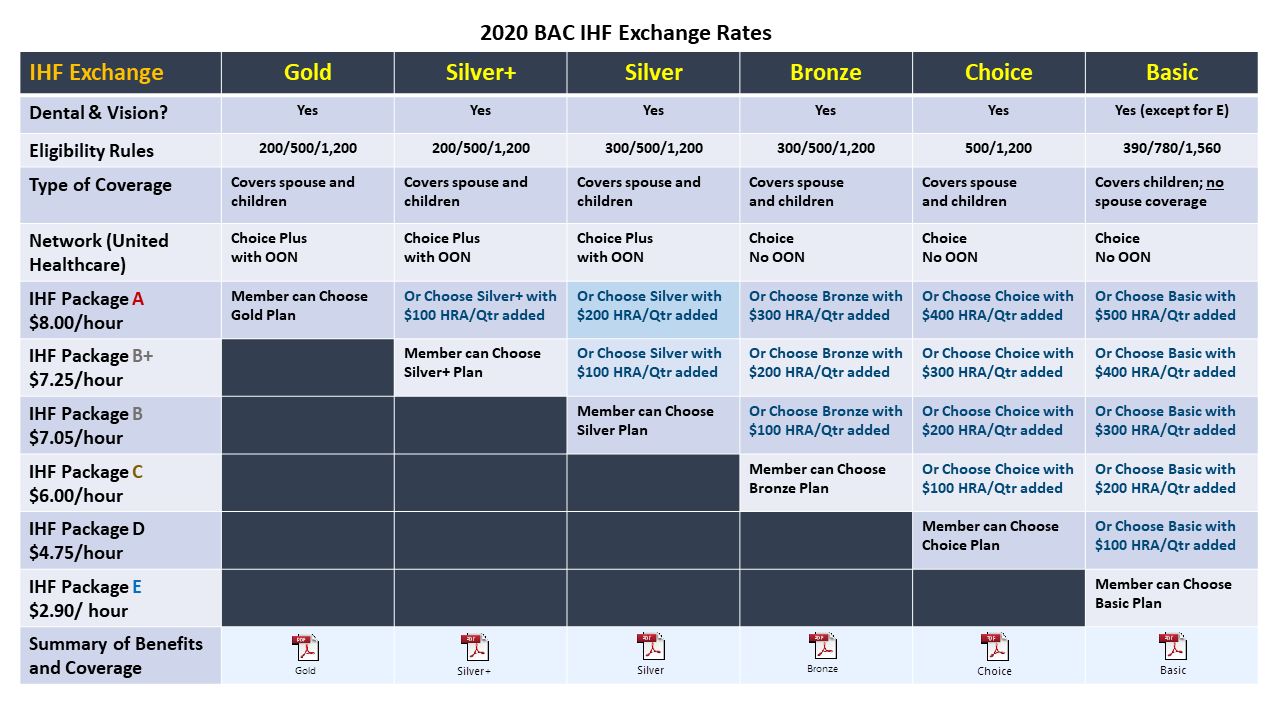
 With the IHF Private Health Exchange, Locals choose from several health and welfare packages. Plans are offered to members in accordance with the IHF Exchange Package that has been negotiated in the Local’s collective bargaining agreement. Members can choose the medical plan within the IHF Exchange Package that best fits the needs of their family. Based on the Local’s agreement, the following additional benefits may be included in the benefit package:
With the IHF Private Health Exchange, Locals choose from several health and welfare packages. Plans are offered to members in accordance with the IHF Exchange Package that has been negotiated in the Local’s collective bargaining agreement. Members can choose the medical plan within the IHF Exchange Package that best fits the needs of their family. Based on the Local’s agreement, the following additional benefits may be included in the benefit package:
- Health Reimbursement Account
- Dental coverage
- Vision coverage
- Life insurance
- Short-term disability
- Vacation benefits
Members in participating Locals become eligible once they meet the eligibility rules outlined in the Plan Document. Members remain eligible for health and welfare benefits as long as they continue to meet the Plan’s quarterly eligibility rules.